Make Social Distancing Restrictions Voluntary

Authors
Steve Trost
Abstract
This paper argues that states should form policy according to rational risk assessment in the face of the COVID-19 pandemic. State and local policy-makers should create a framework that focuses on protecting the most vulnerable. They must also repeal all universal social distancing mandates.
Full Text HTML
Make Social Distancing Restrictions Voluntary
Throughout the COVID pandemic, calls to “follow the science” and “follow the experts” have been loud and frequent. Initially, many experts voiced extreme caution because our knowledge and understanding of the virus was limited, and to ensure that local healthcare facilities were well-equipped to handle any potential influx of seriously-ill COVID patients. As a result of that caution, hospitals nationwide rapidly expanded their critical care capacities while the U.S. Navy and the Army Corps of Engineers demonstrated our nation’s ability to provide additional temporary hospital capacity on very short notice. Fortunately, none of those temporary facilities were ever needed, even in the hardest hit location (New York City).
As we have learned more about the virus and as citizens have experienced firsthand the negative social and health impacts associated with lockdowns and social-distancing mandates, many experts are coming to understand the harmful effects of such mandates are greater than their benefits. The over-11,000 medical and public health scientists who have signed the Great Barrington Declaration (along with over 33,000 medical practitioners) affirm that lockdowns and other restrictions on individual freedoms “cause irreparable damage, with the underprivileged disproportionately harmed.”
Facts Relevant for Developing Effective COVID-19 Policy
The time has come for state and local government officials and governmental-institution leaders to apply solid risk-management principles to their policy-making. To that end, two well-established facts should govern all future COVID-related policy decisions: 1) N95 respirators effectively protect the wearer, and 2) COVID deaths mainly result among the aged and/or infirm. Given the true purpose and effectiveness of properly-worn respirators, and what is best described as the targeted nature of COVID-19, as well as the social costs of extreme across-the-board social distancing mandates, policies specifically targeted to protect vulnerable populations should be implemented – no more, no less.
N95 Respirator Effectiveness
Strong evidentiary support exists regarding the effectiveness of N95 respirators in reducing the wearer’s exposure to virally-contaminated airborne particles (down to 0.3 microns – the SARS-CoV-2 virus, at its largest, is 0.1 microns in size but is usually contained within airborne aerosols and droplets that are larger). For example, a randomized clinical trial of 1,669 healthcare workers investigating continuous use of surgical masks, intermittent use of N95 respirators, and continuous use of N95 respirators demonstrated a significant reduction in viral infections (including coronaviruses) for the wearer with continuous use of N95 respirators, compared to surgical masks.[1]
It should be noted that an N95 respirator is critically different from surgical and cloth masks most people have been regularly wearing during the COVID-19 outbreak. An N95 respirator is designed to provide a tight seal against the wearer’s (clean-shaven) face so that the ONLY air inhaled passes through the filter material.[2] The N95 respirators used in the cited study that were used solely to protect the otherwise unexposed wearers from airborne viral particles, NOT to protect other patients or bystanders.
Surgical masks do not seal against the face, thus allowing unfiltered air to be both inhaled and exhaled. Also, N95 masks not fitted with exhalation valves are prone to malfunction if a wearer’s exhaled breath pushes the mask away from the face enough to temporarily break the seal. Thus, the most effective N95 masks are ONLY about protecting the wearer, NOT about protecting others from an infected wearer.
Asymmetric COVID-19 Fatality Rates
The Infection Fatality Rates (IFRs) of COVID-19 – that is, the percentage of infected individuals who ultimately die from the disease –are very different across different populations (see table below). Especially among the young, and even the middle-aged and healthy, the risks of complications, hospitalization, and fatality from COVID-19 are much less than for seasonal influenza. On the other hand, these same risks for the aged and those with serious comorbidities (such as obesity, hypertension, and diabetes) are considerably greater.
Table 1 – COVID-19 Infection Fatality Rates by Age
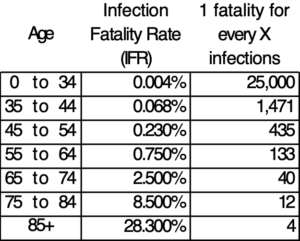
Source: https://doi.org/10.1101/2020.07.23.20160895
Applying the same policies across everyone in a population in response to a virus that has widely varied impacts on different groups within that population can be exceedingly harmful. Those most vulnerable to the virus are not protected as well as they could be, and the underprivileged, who are least able to work or learn remotely, also suffer disproportionately.
Uniform social distancing (i.e. the same levels of social distancing applied to all individuals) essentially guarantees that everyone will be equally likely to get infected with the virus. The problem with this approach is that equal chance of infection coupled with unequal IFRs dramatically shifts the burden onto the vulnerable members of society (the very ones we most need to protect). Although such policies might make everyone feel equally safe, in reality they are grossly inadequate for the safety of some, and wholly unnecessary for the safety of most. This likely leads to MORE fatalities among the vulnerable members of the population.
Consider the ‘hypothetical’ scenario wherein a virus emerges that is inordinately contagious, potentially lethal to a small subset of the population (10%), completely innocuous to a large portion of the population (50%), and vexatious but not unduly harmful to the remainder (40%), and is a type of virus for which a vaccine has never been successfully developed, despite over a decade of previous failed attempts. If such a virus were seemingly random in its selection of who lives and who dies, the societal results would be absolutely devastating—hundreds of millions of fatalities. However, if the virus presented itself in such a way that we could clearly identify the vulnerable 10 percent, the solution would be simple and relatively low-cost: aggressively shield the vulnerable while allowing the virus to ‘do what it does’ throughout the rest of society.
The SARS-CoV-2 virus that causes COVID-19, though dreadfully fatal to a very small subset of the population, has, consistent with the above hypothetical, an unambiguous Achilles heel. We know with considerable precision that, by far, the most vulnerable individuals are those who are elderly (over 75 years of age) and in frail health, along with younger individuals who have specific underlying health problems (e.g. diabetes, obesity, and hypertension). We know that at least 35 percent of the population experience zero symptoms at all (probably closer to 50 percent), with the vast majority of the remainder experiencing full recovery from symptoms within a couple of weeks.
A far better approach to social distancing involves heightened levels that are proportional to an individual’s degree of vulnerability. In other words, the more vulnerable a person is to serious complications or death from the virus, the more aggressively that person should be shielded from all possible sources of infection, albeit in accordance with their own personal risk tolerance.
A Truly Effective COVID-19 Policy
All state, local, and governmental-institution policy-makers should follow these strategically targeted guidelines:
- Eliminate all social distancing mandates (e.g. reduced seating capacity at churches, restaurants, schools, and universities).
- Make N95 respirators (or comparable “fitted masks” whose seals to the face are unlikely to be broken during exhalation) readily available to all vulnerable members of society (including those who may not meet the clinical definition of “vulnerable,” but who nonetheless consider themselves vulnerable).
- Encourage usage of N95 respirators by all vulnerable individuals whenever they are in close contact with any other individual, including members of their own household.
- Encourage symptomatic individuals to self-quarantine until they have been symptom-free for at least 24 hours.
- Establish and enforce specific policies to aggressively protect vulnerable members of the population who rely upon non-family support, such as those in assisted living facilities. For example, require workers in nursing homes to wear N95 respirators at work, as well as when interacting with the general public.
Establish local policies to ease the self-isolation burden of vulnerable members of the population (e.g. work with local churches and community organizations to establish and coordinate a network of community volunteers to provide contact-free grocery delivery to vulnerable individuals).In other words, actively encourage those who are vulnerable or fearful to isolate themselves (and facilitate programs and policies to assist them in doing so) while also allowing those who are willing to accept the risk of infection to knowingly and voluntarily bear that burden. This approach simultaneously reduces the level of COVID health harm to the vulnerable and reduces the level of overall health and economic harm to the non-vulnerable, thereby increasing the economic, mental, and spiritual well-being of all members of society.
Experience at Oklahoma State University serves as a dramatic example of how current policy is ill-advised and how this proposed policy is superior. With many college students having returned to in-person classes across the United States this semester, a distinct increase in cases of COVID-19 among college students has been reported. However, since late July, there have been only three reported COVID-19 fatalities nationwide among college students, even though there have been over 200,000 confirmed cases. That represents an IFR of 0.0015 percent; by comparison, the IFR for seasonal influenza is around 0.15 percent. Meanwhile, on Oklahoma State University’s campus alone, there have been three student suicides since August.
The mental health risks associated with the various governmental and governmental-institution responses to the pandemic far outweigh any benefits, especially in the realm of social-isolation mandates. Universities and schools have universally offered online-only options for students who prefer to avoid in-person classes. Students who are fearful of the virus have been given the option to voluntarily self-isolate, which is laudable. With that safeguard in place, those who choose to voluntarily socialize with their community and support groups should be able to do so without restriction.
Conclusion
Any reduction of individual liberty in the name of public safety must be significantly beneficial to public safety. Early governmental policy on social distancing was arguably defensible as knowledge was limited and risks were perceived to be extremely high. However, given what we know now, mandated social distancing for all does less to reduce COVID-19 deaths than the voluntary wearing of N95 respirator masks by the vulnerable. Further, the non-COVID costs of social distancing have proven extremely high, and disproportionately affect the underprivileged.
Thus, all state, local, and governmental-institution social-distancing mandates should cease immediately, and future pandemic-mitigation efforts should exclusively target shielding and protecting the vulnerable among us.
[1] Mary T. Bessesen, Connie Savor-Price, Michael Simberkoff, Nicholas G. Reich, Andrew T. Pavia, and Lewis J. Radonovich, “N95 Respirators or Surgical Masks to Protect Healthcare Workers against Respirator Infections: Are We There Yet?” American Journal of Respiratory and Critical Care Medicine, 187, no. 9 (May 2013): pp 960–966, https://www.atsjournals.org/doi/full/10.1164/rccm.201303-0581ED.
[2] “N95 Respirators, Surgical Masks, and Face Masks,” U.S. Food & Drug Administration, website, https://www.fda.gov/medical-devices/personal-protective-equipment-infection-control/n95-respirators-surgical-masks-and-face-masks.